Responsible IVF: The missed opportunity of abnormally fertilised embryos
As a fertility patient you might be told that some of your embryos are abnormally fertilised and therefore can't be used. In this article I describe why that isn't always true because our understanding of fertilisation has grown.

As a fertility patient you might be told that some of your embryos are abnormally fertilised and therefore can't be used. In this article I describe why that isn't always true. Our understanding of fertilisation has grown. It is no longer satisfactory for you to receive a potentially detrimental outcome because a clinic doesn't use the appropriate technology.
However, the challenge is that many clinics are up against budget constraints, typically those in the NHS. I'm not here to bash those clinics. I'm here to amplify this issue so you can ask your clinic questions to help you make informed choices. Note, to account for new knowledge, abnormal fertilisation is now called atypical fertilisation. However, clinics will most likely still refer to them as abnormally fertilised embryos.
When selecting a clinic many people will have other embryos to use, but for those with a low ovarian reserve they need to think about how a clinic deals with atypical fertilised embryos.
Before I offer six questions to ask your clinic when your embryos are abnormally fertilised, let's dive into the science.
The difference between atypical and normal fertilisation
Within nearly every human cell lies a single nucleus, which contains all the information that makes you uniquely you. A typical nucleus is home to 46 chromosomes arranged in 23 pairs. This is a state known as diploid – two copies of each.
The egg and sperm (gamete) are made by dividing a germ cell containing 46 chromosomes, in half. Thus each egg and sperm contain only 23 chromosomes. A state known as haploid – one of each.
When an egg meets a sperm and fertilisation occurs correctly, Those 23 chromosomes from each gamete meet their counterpart of the pair, and hence this new entity is now considered diploid. When all the chromosome pairs are present and in the correct number, it is known as diploid euploid. When there is an extra chromosome making the embryo abnormal, the entity is still known as diploid but then it is called diploid aneuploid.
At the very beginning, before the first cellular division occurs, a fertilised embryo, is known as a zygote. A zygote, although it is diploid, it is also the only single cell in human beings that contains two nucleus'. That is because, until they fuse, the nucleus' from the sperm head and the egg itself show up as being distinctly separate nuclei. These nucleus's derived from a gamete are termed pronuclei (PN).
It has long been believed that for an embryo to be considered normally fertilised and therefore a viable potential to take forward and grow, there should be two – and only two – pronuclei seen. We call them a 2PN. Anything outside of this visual norm, such as too many PN's (3PN) or too few (1PN), has always been considered abnormal, and in the majority of clinics, these embryos are discarded and not cultured (grown on) any further.
Deciphering the pronuclei (PN)
Watch this timelapse video of the first 28 hours of a human embryo and I'll then explain what's happening.
A timelapse video of the first 28 hours of a human embryo
When fertilisation starts, about 1-4 hours after the sperm has entered the egg, the egg spits out a small structure called a 2nd polar body (PB). For an egg to be considered mature it has to have one polar body already, that sits in the space between the actual egg and the shell called the perivitilline space. The second extrusion is necessary for the fertilisation process to be initiated. This is not the post for me to go into the why and what the second polar body is, this is not a molecular biology lecture, and I'm trying to keep it simple. So on this one I ask that you trust me that this is just what it is.
The 2nd Polar body being extruded can be seen when the embryos are under timelapse, but it is far from an exact science and fertilisation cannot be determined simply on the presence or absence of this second PB. Because as quickly as it appears, it can also fragment, and so although seeing it is important, it does not give us enough information.
So what happens next? It is generally accepted that the pronuclei (PN's) appear at approximately 5-10 hours after insemination. Insemination is the process by which the sperm and egg are introduced to each other. I appreciate makes it sound a bit like they are on a date 😉! Insemination will be either by IVF, where the sperm and eggs are mixed together and left to their own devices, or by ICSI, where a single sperm is injected into each mature egg.
The PN's, once appeared, usually persist until around 22-26 hours after insemination, at which point they fuse and disappear, usually at exactly the same time, in a process called syngamy. The state of syngamy can last anything from 30- 120 minutes. At the point of syngamy it should be said that the embryos look exactly like unfertilised eggs again for that period of time. At the end of the syngamy phase, the first cell division should occur, bringing about a 2-cell in embryos developing normally.
What does an atypical embryo really mean?
Anything that doesn't look like the textbooks is considered atypical. So if normal is called a 2PN, lets talk about what else we see and why this happens.
Most clinics perform fertilisation checks on eggs at approximately 18-20 hours from the point that they have been inseminated with sperm, normally the morning after the day that the eggs were collected/thawed. If ICSI has been performed, and the eggs are placed under timelapse video, then it doesn't matter when they are look at again. An embryologist will simply press play and watch all the events unfold.
But if IVF has been performed, or the clinic doesn't have timelapse, the clinic relies on accurate time evaluation of all eggs & embryos, to 'see' what is meant to be seen. This also relies on all embryos behaving like a textbook description yet sadly not all embryos have read the textbook!
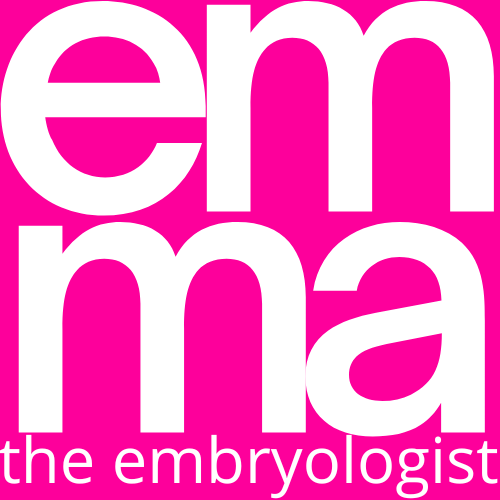
1PN
In the picture above only one nucleus can be seen. This could mean that fertilisation has not occurred correctly and this is a haploid cell. If that's the case then this will most likely not grow, if it does it will most likely not result in a pregnancy. But if I then tell you that up to 60% of these are known to be diploid and potentially normal, should we really be discarding them when the outcome of using them is not known to be harmful? What are the reasons that we can't see the second nucleus.
- The nucleus' are sat on top of each other and could be just indistinguishable from one another.
- Syngamy has happened in an asynchronous manner, meaning that one of them has disappeared earlier then the other one, at the point of checking, we see this a lot in timelapse.
- Solo activation occurs by the egg without sperm fusion.
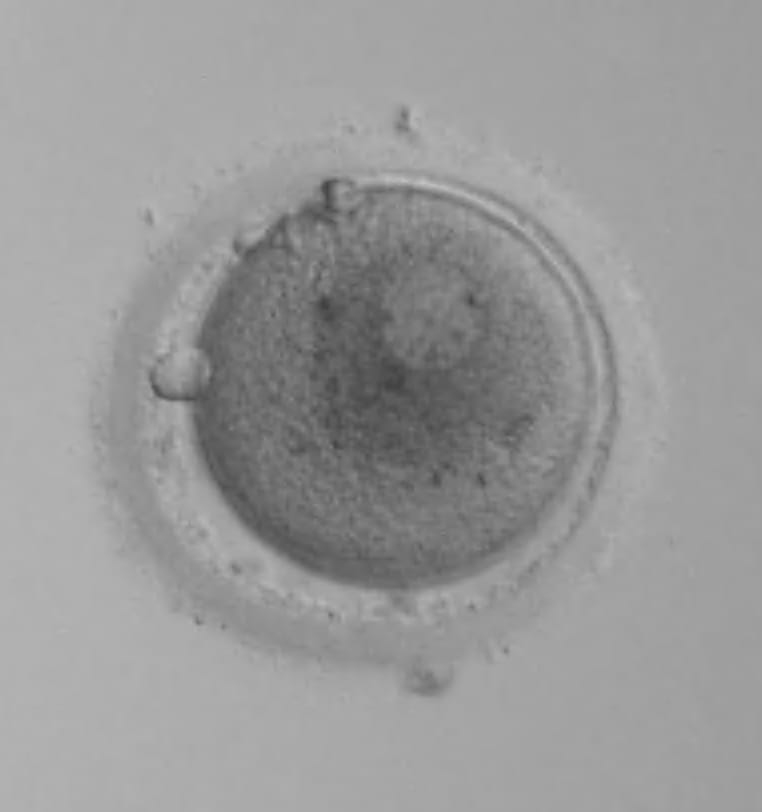
3PN
In the picture above three nucleus' can be seen very clearly, they are all roughly the same size and this is an embryo that is discarded in most clinics immediately. If each of the nucleus's contain a full set of chromosomes this is known as triploidy. This can happen in IVF cases where two sperm get into the egg instead of one, a situation called polyspermy.
If it is a true triploidy embryo this would mean there are three copies of all chromosomes instead of two. If these embryos create pregnancies they can result in very dangerous partial molar pregnancies that in extreme cases can become cancerous. So to use these without confirmation of genetics would be negligent.
However these aren't always truly triploid and in a small percentage they have been found to be diploid normal embryos after genetic testing.
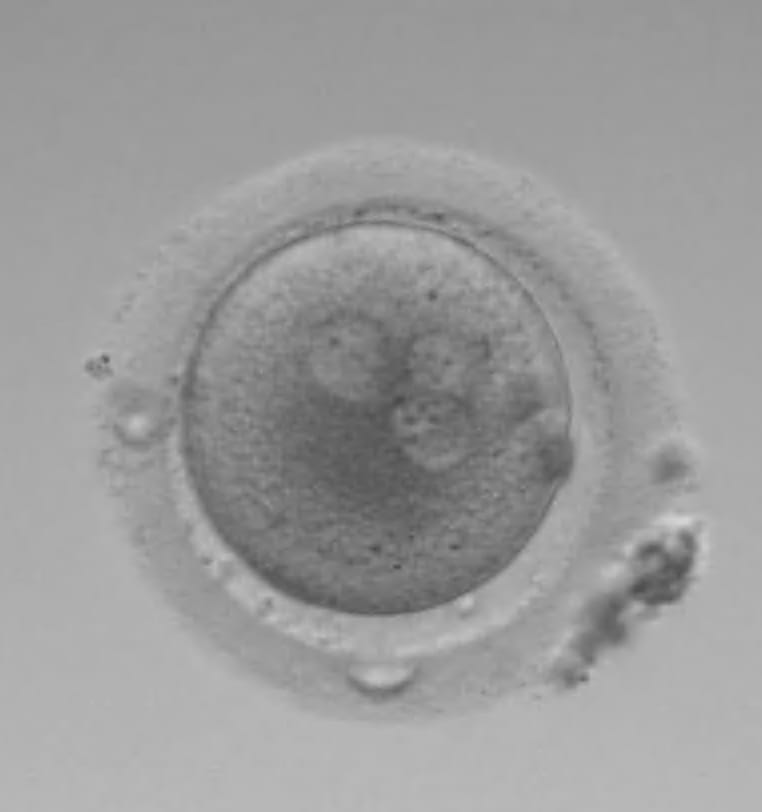
2.2PN/2.1PN
In the picture above, on the left, you can see two normally sized nucleus's and two smaller nucleus'. In the picture on the right, there is two normally sized nucleus and one smaller. The size of the nucleus' is important here. For a long time the picture on the left, would have been called a 4PN. The picture on the right, a 3PN. Both situations would have ended with them being discarded. But we now know that the size of the nucleus' are important, and we have changed the way we refer to them.
The possibility of either of these being an absolute triploid entity is too high for us to use these embryos safely, without testing first.
Note the 2.1PN embryo on the right grew into a beautiful blastocyst, underwent PGT-A to determine it being normal, and was transferred, resulting in a successful pregnancy and live birth.
0PN
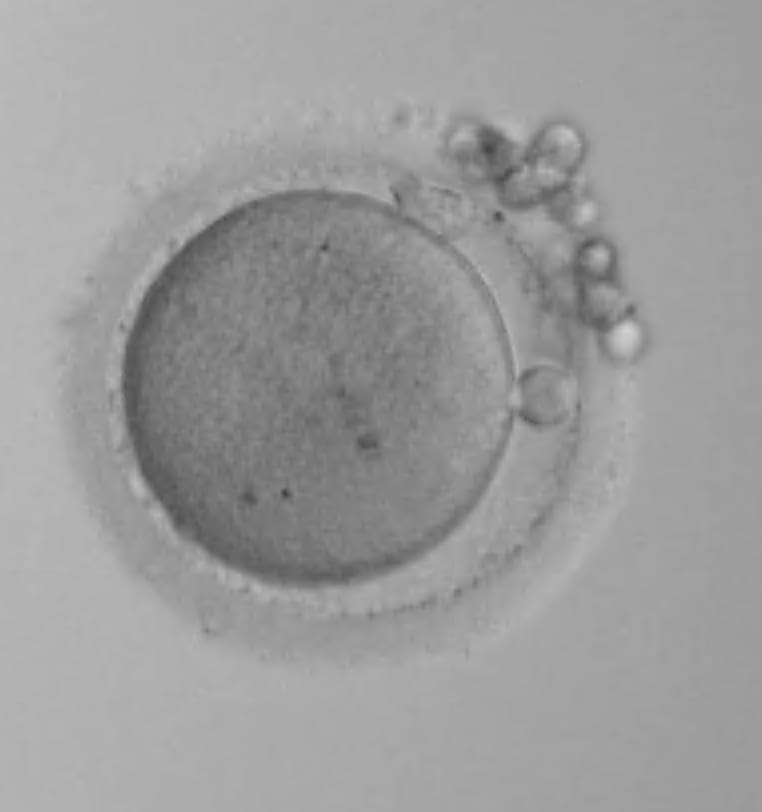
The picture above looks like an unfertilised egg, but it has the two polar bodies that are needed to be seen, and so we call this a 0PN. These are the normal embryos that I think are discarded incorrectly more than any other type.
When these happen under timelapse they are normally not viable. They do not normally grow. But if there is not timelapse, there is a very sizeable possibility that this is actually in syngamy early and thus the PN's have already disappeared before the time of checking.
From my own work I believe that between 3-5% of embryos go into syngamy before 18 hours when the embryologists do their checks. So are we just missing what we need to see?
Six questions to ask your clinic when your embryos are abnormally fertilised
Be brave and ask your clinic the following questions to get a sense of how they deal with abnormally fertilised embryos. As a reminder, it may be that they just can't provide the right service for your needs as they are not set up to do so.
- What does your clinic do with abnormally fertilised embryos?
- Does your clinic offer PGT-A testing?
- Does your clinic have timelapse?
- What time does your clinic perform fertilisation checks?
- Does your PGT-A testing lab enable molecular fertilisation checking?
- Will you allow me to freeze embryos regardless of the visual fertilisation status?
Keep everything and allow them to grow
For me – and what we do at The Evewell – is to keep everything and allow them to grow to see if these embryos can reach the blastocyst stage. This is a stage of embryo development that occurs about five or six days after fertilisation, when the embryo is ready for implantation. If they do reach the blastocyst stage, the embryologists are in a position to perform testing on these embryos, before freezing them, to ascertain whether they are safe to use in embryo transfer.
PGT-A testing of embryos is now so advanced that it is able to determine whether any embryo, where a biopsy is taken at the blastocyst stage is diploid, haploid, triploid, aneuploid and euploid. This is considered a way to save these embryos from discard, as it enables a molecular fertilisation check to be done. In cases where patients have very few eggs and all they have is considered abnormally fertilised embryos, we have to give them the option to use the technology to be sure, before we discard anything.
The fate of half of all embryos are incorrectly determined
Multiple studies aim to understand the percentage chance of embryos being genetically 'normal' when they do not show the correct visual signs at the beginning. One article pulled together all this information and suggests differing chances of these embryos being diploid. But as with everything, it is treatment and age related and it is incredibly nuanced. The paper suggests that through visual assessment alone we are incorrectly interpreting, and thus, determining the fate of these embryos as much as 50% of the time.
This is an incredibly important breakthrough in our understandings. The problem we now face is that many clinics are not able to offer the necessary testing to determine whether embryos with abnormal visuals can be safely used or not.
A parting thought about PGT-A and the HFEA
The HFEA’s claim that PGT-A won’t increase the number of usable embryos is a blatant oversight. My personal experience, and countless others, tell a different story. In fact, PGT-A can be a lifeline, especially for those with limited embryo options. It’s time to challenge the status quo and recognise the true potential of this technology.